South African Medical Professionals Opposing Harmful Drugs and Surgeries
The Southern African HIV Clinicians Society (SAHCS) Position Statement on the provision of care for adolescents with gender incongruence has serious shortcomings.
On 26 August 2024 the Southern African HIV Clinicians Society (SAHCS) published a position statement on the provision of care for adolescents with gender incongruence. The purpose of this statement appears to be to defend their Gender Affirming Healthcare Guideline (GAHG) which was published in 2021.
The background to this development is the engagement between First Do No Harm Southern Africa (FDNHSA) and the SAHCS regarding their GAHG . The first discussion between FDNHSA and the executive of the SAHCS took place on 29 April 2024.
Following this, and in response to the specific request of SAHCS executive members, on 6 May 2024 FDNHSA sent the SAHCS a letter outlining concerns about their GAHG with regard to the medicalising treatments of children and adolescents contained in the guideline.
The SAHCS did not provide FDNHSA with any response, despite several follow up emails. Three and a half months later, on 26 August 2024, they produced the Southern African HIV Clinicians Society (SAHCS) Position Statement on the provision of care for adolescents with gender incongruence, which they posted on their website:
The position statement notes there have been new developments regarding GAHC recommendations, including a
“2024 review conducted by a team of medical professionals in the United Kingdom that raised concerns regarding the availability of gender-affirming treatment, particularly in relation on to puberty blockers and hormone therapy for adolescents”.
There is no further discussion or acknowledgment of the significance of the Cass Review which concluded that the use of puberty blockers and cross sex hormones in children as part of a “gender affirming” care package, has been based on “wholly inadequate evidence”. The Cass Review has been a significant international gamechanger, marking the end of the era of unquestioning “gender-affirming care”, a medicalized approach to the treatment of young people with gender-related distress.
While the report was commissioned by the NHS to provide specific direction to gender services in the UK, the evidence collated, synthesised and presented is globally relevant, and is based on 4 years of rigorous research backed by 8 systematic reviews.
The SAHCS do not appear to take the findings or recommendations of the Cass review seriously, despite the fact that this is the best quality evidence currently available globally regarding the care of children and adolescents. Their position statement instead refers to World Health Organisation (WHO) guidelines that are under development, and state that they will wait for these guidelines to be released.
There are two major issues of concern regarding the SAHCS position statement:
The WHO has clearly stated that they will not be producing guidelines about “gender affirming care” for children and adolescents.
Why will the [WHO] guideline only cover adults and not also children or adolescents?
The scope will cover adults only and not address the needs of children and adolescents, because on review, the evidence base for children and adolescents is limited and variable regarding the longer-term outcomes of gender affirming care for children and adolescents.
2. The process of the WHO producing guidelines for adults has been criticised due to conflict of interest in the guideline group, lack of proper due process and the composition of the guideline group which contains members who are related to the World Professional Association of Transgender Health (WPATH), which has lost credibility due to its unethical actions. This has been summarized by Society for Evidence Based Gender Medicine:
“WPATH members involved in the production of the WHO guidelines were directly involved in suppressing unfavorable evidence related to the availability of cross-sex hormones in the process of creating their society’s official guidelines: WPATH Standards of Care 8 (SOC8). Since the availability of cross-sex hormones is a key topic for the upcoming WHO guideline, this sets a deeply troubling context for WHO’s current efforts. In our most recent response to WHO, we expressed our renewed concern with the WHO GDG composition in light of the documents disclosed in a U.S. court case, which reveal that WPATH undertook explicit steps to suppress and manipulate evidence in the space of transgender health”
Currently, the SAHCS GAHG recommends as follows “If an adolescent desires puberty blocking medication, hormone therapy or surgery, the informed consent process requires …” . This is a clear endorsement of a fully medicalised approach, which is what the Cass review cautions against.
The WHO is not going to produce guidelines to protect vulnerable children and adolescents. South African health care authorities, professional societies and associations need to take responsibility for protecting children and adolescents against medical practices which have a poor evidence base and can result in serious harm.
In conclusion
We call on the SAHCS to make a clear statement that puberty blockers and cross sex hormones for children and adolescents remain experimental and should not be prescribed except within the bounds of clinical research.
FDNHSA letter to the SAHCS sent in May 2024, specifying our concerns with the GAHG, including the process of producing the guideline:
To: South African HIV Clinicians Society Board
From: First Do No Harm Southern Africa
6th May 2024
Concerns about the South African HIV Clinicians Society (SAHCS) Gender Affirming Healthcare Guideline (GAHG), in the light of the Cass Review
This letter is a follow up on a discussion between some members of the Board of the South African HIV Clinicians Society (SAHCS) and representatives of First Do No Harm SA (FDNHSA) on 29th April 2024. It was suggested at the end of the meeting that FDNHSA send a formal letter to the Board highlighting their concerns as well as the recommendations which were briefly discussed.
Background
Over the last few years there has been a dramatic increase in children and adolescents being diagnosed with gender dysphoria, gender incongruence or gender distress in many countries, including South Africa. The best approach for caring for this vulnerable group is globally contested and remains controversial. Much needed, evidence-based direction has recently been provided.
On the 10th April 2024 the Cass Review was released by the National Health Service (NHS) in the United Kingdom (UK).(1) Led by paediatrician Dr Hilary Cass, the review publishes the findings of and recommendations arising from a 4-year investigation into how the NHS provided care to children and young people with gender dysphoria. The systematic reviews undertaken by the University of York as part of the review’s independent evidence gathering process are the largest and most comprehensive to date. The York investigators looked at 237 papers from 18 countries, providing information on a total of 113,269 children and adolescents. When the investigators reviewed guidelines used around the world, the SAHCS GAHG was included.
The Cass Review, accompanied by nine studies(2-10 ) eight of which were systematic reviews of evidence, has been a significant “gamechanger”, marking the end of the era of unquestioning “gender-affirming care”, a medicalized approach to the treatment of young people with gender-related distress. While the report was commissioned by the NHS to provide specific direction to gender services in the UK, the evidence collated, synthesised and presented is globally relevant. As stated by the UN Special Rapporteur on violence against women and girls, Reem Alsalem on 24th April 2024:
“The Cass review findings and recommendations are seminal, and its implications go beyond the United Kingdom. While the Cass Review may not have framed its conclusions and findings explicitly in human rights language, it has – in my view – very clearly shown the devastating consequences that policies on gender treatments have had on human rights of children, including girls. These policies have breached fundamental principles, such as the need to uphold the best interest of the child in all decisions that affect their lives, and the right of children to the highest attainable standards of health”.(11)
The Cass Review concludes that ‘gender affirming’ medical treatments, which include providing puberty blockers and cross-sex hormones, are based on ‘wholly inadequate evidence’. Doctors are usually extremely cautious when adopting new treatments, but Cass said ‘quite the reverse happened in the field of gender care for children’. Instead, thousands of children were put on an unproven medical pathway. Worse, medical professionals seemed largely uninterested in uncovering the side effects and long-term risks of these drugs. Of great concern was that Cass highlighted that all but one adult gender clinic(12) refused to share patient data that would allow her team to study how childhood transitioners fared as adults. This made it virtually impossible to research the longer-term consequences of transitioning. It also raises concerns about the care provided in adult gender clinics and the reasons for the lack of transparency.
The Cass Review arises from the UK context, but has relevance for South Africa
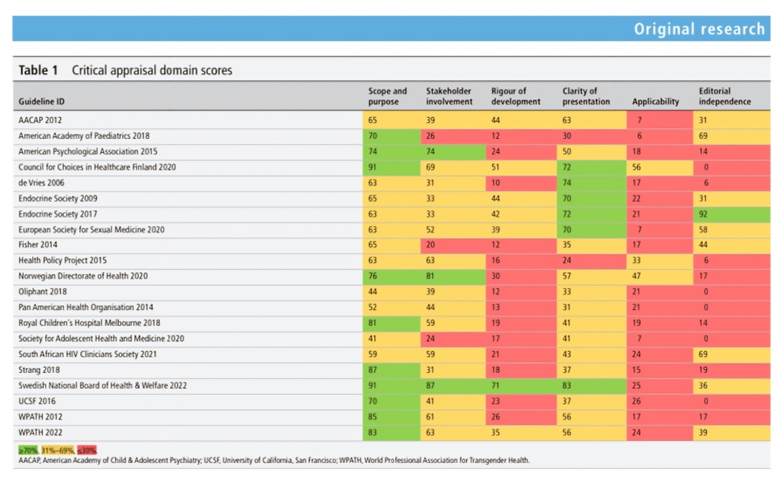
There have been attempts to challenge the value and validity of the Cass review, with some detractors claiming that the Cass review is focused on the UK context and thus has no relevance for South Africa. Nine new systematic reviews have been published in the reputable Archives of Disease in Childhood. The Cass Review draws on the results of these(2-10). Two of the 9 reviews looked at 23 guidelines from across the world.(8-9) The SAHCS GAHG was included in both.
In the review “Clinical guidelines for children and adolescents experiencing gender dysphoria or incongruence: a systematic review of guideline quality (part 1)”(8), nine of the reviewed guidelines were noted to have been adopted by professional bodies, the SAHIV Clinicians Society being one of the nine to do this. The SAHCS GAHG scored particularly poorly in ‘rigour of development’ and in ‘applicability’.
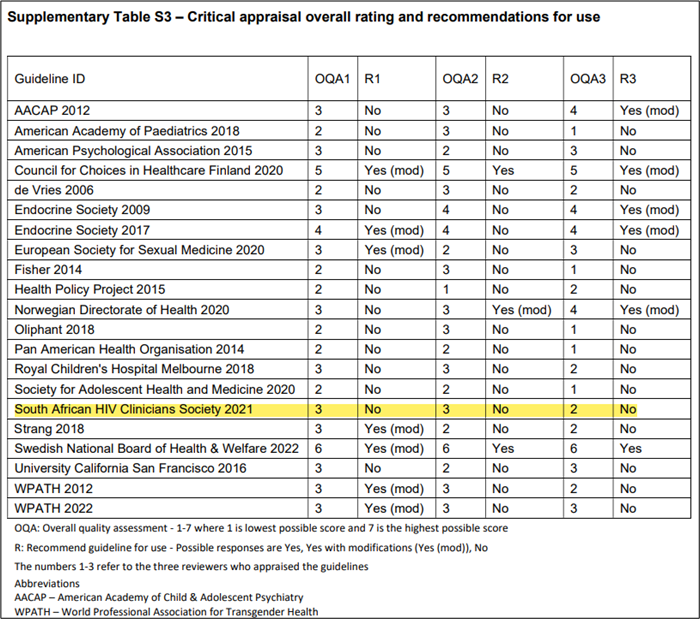
Further, in the supplementary material for this review,(8) not one of the 3 reviewers was able to recommend the SAHCS GAHG for use.
In the review “Clinical guidelines for children and adolescents experiencing gender dysphoria or incongruence: a systematic review of recommendations (part 2)”(9), shortcomings of the SAHCS GAHG are noted on Table 1 page 5 of the report, including:
Lack of discussion on the assessment domain of body image.
Lack of discussion on the assessment domain of sexuality or sexual orientation.
Lack of discussion on the assessment domain of sexual functioning or health.
Lack of discussion on the assessment domain of cognitive functioning/ intelligence/ maturity.
Lack of discussion on the assessment domain of physical health or conditions.(8)
This review also highlighted that the SAHCS GAHG guideline contains no lower age limit recommendation for surgery (bilateral mastectomy, phalloplasty, vaginoplasty et al.) in adolescents.
The conclusion of this systematic review(8) was:
“Published guidance recommends a care pathway for children and adolescents experiencing gender dysphoria/incongruence for which there is limited evidence about benefits and risks, and long-term effects. Divergence of recommendations in recent guidelines suggest there is no current consensus about the purpose and process of assessment, or about when psychosocial care or hormonal interventions should be offered and on what basis.”(8)
The Southern African HIV Clinicians Society (SAHCS) Gender Affirming Healthcare Guideline (GAHG)
The Southern African HIV Clinicians Society (SAHCS) has always been at the forefront HIV care by providing leadership in South Africa at a very difficult time in our history. Over the last 25 years, the SAHCS has co-ordinated continuous medical education for all levels of healthcare workers and, with the support of local and international clinical HIV experts, has been committed to improving HIV/TB care in Southern Africa. The organization focusses on capacity building, guideline development, high quality virtual learning, mentorship programs for HCWs, and providing a network for HIV practitioners. The careful interpretation and use of data for programmatic improvements are core to SAHCS. SAHCS has dedicated itself to working with the National Department of Health, provincial and district health bodies, using epidemiologic, program and process data for comprehensive, quality, cost-effective, and tailored interventions.
The SAHCS GAHG guideline, published in 2021, is a curious departure from the previous work of the SAHCS. ‘Gender medicine’ is not part of the core business of the Society. ‘Gender medicine’ is new area of medical care.
In an article in the SA Family Practice Journal, 3 of whose authors also wrote the SAHCS GAHG, the authors state:
“Gender Affirming Healthcare is a relatively new field in medicine and the guideline hopes to address the significant gaps in knowledge and skills of healthcare providers in providing GAHC to transgender and gender diverse (TGD) people”(13)
The SAHCS GAHG includes guidance for both adults and children. It recommends “gender affirming care” starting with social transition and progressing to puberty blockers, cross sex hormones and surgery for children and adolescents.
While we have an overall concern about the general recommendation for “gender affirming” care, we highlight the following specific issues in the guidelines:
The role of parents:
The Convention on the Rights of the Child recognizes the unique importance of parents, holding States accountable to respect the “rights and duties of parents,”(Article 5), and referring to the child’s right “to know and be cared for” by parents, (Article 7 (1)). Parents, in Article 18(1), are acknowledged to “have the primary responsibility for the upbringing and development of the child.” This is because the child’s best interests are the parents’ core concern.
The SAHCS GAHG does not position the child firmly within a family. Section 2.3 of the “shorter version” starts with quoting from the Children’s Act, and states that a child may consent to “medical treatment” from the age of 12 and goes on to define “medical treatment” to be a “manifestation of the right to health”. It then goes on to state “if an adolescent desires puberty blocking medication, HT (hormone treatment) or surgery”, as if to define this as “medical treatment”. This section finishes with “it is recommended that both parents and legal guardians be included in this process wherever possible…” (14)
The expanded version of the GAHG clarifies your guideline’s stance on parents/guardians:
“A situation may arise where an adolescent requests assessment and intervention or a referral to an MHP [Mental Health Care Practitioner] is received from the school, or any other source other than the parents/legal guardians, and where attempts to engage the parents/legal guardians are unsuccessful … Another situation may arise where the parents of the TGD [Transgender] adolescent disagree about GAHC [Gender Affirming Health Care] for their child. If there is reason to believe that the parents/legal guardians are not acting in the best interest of the adolescent, as above with younger children, appropriate referral should take place.”(15)
These recommendations imply that parents who do not agree with the “gender affirming” approach may not be acting in the best interests of their children. It minimizes the importance and role of parents in decision making on an extremely important issue in the life of the child. Given the risk of harm, parents should be cautious and concerned.
Under this recommendation, it would be possible for a 12-year-old to consent to puberty blockers, cross sex hormones, and surgery, which are likely to result in reproductive sterility, sexual dysfunction, inability to breastfeed among other serious consequences – which a 12 year old cannot properly understand. And this is made possible if a gender affirming practitioner deems it ‘impossible’ to include the parents or asserts that the parents are not acting in the child’s best interest.
Surgical interventions and psychological evaluations:
Gender affirming care for children and adolescents in the SAHCS GAHG includes surgery. Gender affirming clinicians often refer to “top surgery” and “bottom surgery”. These euphemisms misinform and confuse practitioners, parents and children. These ‘surgeries’ include bilateral mastectomy, removal of pelvic organs, and constructing pseudo penises or vaginas (some surgeons create pseudo-vaginas and leave the penis; some offer nullification surgery, removing all secondary sex traits – breasts, nipples, penis, vagina). Obviously, all carry serious risks, including sexual dysfunction and sterility. How can children and adolescents (and their parents) fully grasp the implications?
Further, the SAHCS GAHG states:
“If the client is able to consent, then their autonomy should be respected and facilitated, and it is recommended that in the case of an MHP writing a referral letter to a surgeon, this is written in collaboration with the client in a participatory way. We note that the WPATH SoC-7 states that a client should have two independent psychological evaluations prior to surgery. However, it has been convincingly argued that this is not necessary for all clients.” (15)
With high rates of pre-existing psychiatric conditions and growing rates of regret and detransition occurring after “gender affirming’’ surgeries have been carried out – combined with the severity and irreversibly of harms from these surgeries, and low-quality evidence of any benefit – thorough psychological and psychiatric evaluation before surgery should be recommended as essential.
Non-maleficence and beneficence are central tenets of medical ethics. There is no evidence that surgery for adolescents with gender dysphoria provides benefit and there is good evidence that it causes severe harm.
Informed consent in minors, detransitioners and medico-legal risk
The GAHG does not engage substantially with the critical issue of informed consent relating to the ability of children and adolescents with developing minds and brains to be able to consent to medicalizing interventions with long-term and mostly permanent effects.(16-18) Internationally, there is a growing number of detransitioners, those who made a decision while young to embark on the “gender affirming” pathway and later regretted this decision. The SAHCS GAHG does not provide guidance regarding the care of detransitioners. The growing number of detransitioners in counties where the “gender affirming care” medicalised approach has been followed over the last decade has been accompanied by many high-profile court cases being brought against doctors (19-27), a fact that South African doctors need to be aware of. In terms of medico-legal risk, the SAHCS may also be at medico-legal risk if a detransitioner’s doctor said that they were following the GAHG in providing “gender affirming” care in a child or adolescent.
The importance of an evidence-based guideline
A health care guideline produced by a professional medical body such as the SAHCS carries significant weight for its members and for the community at large. It is therefore important that the guideline is developed in a rigorous, scientific, and professional manner, and is based on high quality evidence especially when the long-term health of vulnerable children and adolescents is at stake.
The current SAHCS GAHG is not supported by high-quality evidence (2-10,28-31) and directly contradicts statements made by several national health systems, including the NHS, Finland, and Sweden.(1,28,29,32-34)
Finland, following their systematic review of evidence, emphasizes the need for an adolescent to first complete their developmental tasks, and for other psychiatric illnesses to have stabilized or improved before a gender identity assessment will be considered. The statement reads,
If an adolescent experiencing gender anxiety has had or has concomitant psychiatric symptoms requiring specialized care, in case the need for it continues after the psychiatric symptoms have yielded and the adolescent development tasks’ progress has normalized, it is possible to consider gender identity examinations.”(28)
In the United Kingdom, the use of puberty blockers is now restricted to a research setting and will only be prescribed within the confines of a proper clinical trial.(1,33)
Until recently, most societies or organisations (including PATHSA, the Psychological Society of South Africa (PsySSA), the South African Society of Psychiatrists (SASOP)) that follow and/or espouse the “gender affirming” model of care for transgender people follow the World Professional Association for Transgender Health (WPATH) Standards of Care (SOC) 7/8. When concerns are raised with WPATH on the quality of their guideline, one response has been to emphasize that it is a ‘standard of care’, and not a ‘guideline’. This is disingenuous. If the SOC is the functional guideline, it needs to be evaluated for its quality in the same manner that any other guideline is evaluated.
Evidence based medicine experts have developed standardized analytical tools for evaluating guidelines. One such is the AGREE II tool (Brouwers et al. 2010)(35). AGREE II evaluates the development processes of and underpinning evidence used for guideline. The domains of the AGREE II tool that are of particular interest in the case of WPATH SOC 7 are the following:
Domain 2: Stakeholder involvement
Domain 3: Rigour of development
Domain 6: Editorial independence.
Evaluation of the WPATH SOC 7 (and now 8) with the AGREE II tool shows:
Stakeholder Involvement: WPATH has failed to involve or listen to anyone that does not follow or, in effect, approve of the gender affirming model. No other options for care are considered. Therefore, no alternative treatment pathways, based on the specific circumstances of the patient, are offered.
Rigour of Development: In all 8 items in the tool, WPATH fails to show that quality evidence was used to inform their recommendations. The recommendations in some cases directly contradict the evidence quoted. The heart and backbone of any guideline is based on the evidence gathered to support the recommendations. A failure in this domain should be seen as a failure of the guideline as whole.
Editorial Independence: The development of WPATH SOC 7 and 8 is known to be compromised. WPATH is a self-appointed body that includes transgender people (or those with close family members who are transgender). Their guidelines are best explained as being developed by themselves, for themselves, and for like-minded people with transgender ideation. Also, journals and companies that push for the affirming model offer financial incentives to WPATH committee members (MacRichards, 2019)(36). In which other mental health (or any other medical) condition guideline is the patient the main developer of the guideline, and is such partiality allowed?
WPATH SOC 7 and 8 fail significantly in all domains needed to be regarded as quality guidelines. They are now discredited, although it has taken a long time for critiques of WPATH to be taken seriously. Any medical or psychiatric society (such as yours) that continues to base their guidelines or position statements on the WPATH SOC 7 or 8 should think very carefully about their commitment to evidence and unbiased patient care.
For further insight into the workings of, evidence base used by, and professionalism in WPATH, see:
The SAHCS GAHG is rooted in the WPATH SOC7. One of the two guideline committee chairs, is a current member of the Board of Directors of WPATH.
Conflict of interest and bias in guideline development
Guideline committees should have impartial professionals such as research methodologists to assist in collating medical evidence in an impartial way and conflicts of interest must be addressed. Sometimes members might have to be excluded due to conflicts of interest.
Conflicts of interest can be financial, personal, intellectual or academic. For a topic such as management of transgender ideation in children and adolescents which is at high risk of bias, we would suggest attention be given to possible conflicts of interest in the guideline development group. For example, if a child psychiatrist is actively engaged in directing large numbers of families to socially ‘transition’ their children and openly declaring doing so, this would make it difficult for them being able to describe the concretising and risky nature of social transition. Such a practitioner would be significantly biased and likely unable to impartially use emerging evidence on social transition to inform a guideline.
Likewise, if a professional has a close friend or family member that is receiving ‘gender affirming care’, this could be a significant conflict of interest.
The same is likely for committee members who themselves identify as transgender.
Conflicts of interest have not been adequately addressed in the development of the SAHCS GAHG, which explicitly states that it is committed to “upholding a strength-based perspective that values and respects the experiences of TGD clients”. The section on methodology states that:
“The guideline development committee comprised 17 people, chaired by Dr Anastacia Tomson and Rev. Chris/tine McLachlan, which was inclusive, with representation of providers, advocates and civil society organisations in the TGD space, and many with personal experience as a TGD client. Development was predicated on the necessity to amplify the voices of those within the TGD community in order to better meet their needs, rather than presuming that healthcare providers can address those needs alone. ….The committee worked from a gender-affirming, non-gatekeeping, depathologising perspective using a participatory approach that centres on the TGD client’s agency and humanity, and upholds their dignity.”
In a British Medical Journal report ‘Gender dysphoria in young people is rising—and so is professional disagreement’, the following is stated:
“”The brief history of guidelines is that, going back more than 30 years ago, experts would write articles and so on about what people should do. But formal guidelines as we think of them now were seldom or non-existent,” says Gordon Guyatt, distinguished professor in the Department of Health Research Methods, Evidence, and Impact at McMaster University, Ontario.That led to the movement towards developing criteria for what makes a “trustworthy guideline,” of which Guyatt was a part. One pillar of this, he told The BMJ, is that they “are based on systematic review of the relevant evidence,” for which there are also now standards, as opposed to a traditional narrative literature review in which “a bunch of experts write whatever they felt like using no particular standards and no particular structure.” Mark Helfand, professor of medical informatics and clinical epidemiology at Oregon Health and Science University, says, “An evidence-based recommendation requires two steps.” First, “an unbiased, thorough, critical systematic review of all the relevant evidence.” Second, “some commitment to link the strength of the recommendations to the quality of the evidence.””(38)
The SAHCS GAHG does neither.
What the Cass Review means for the SAHCS GAHG, and for South African children
A) Social transition for children and adolescents with gender dysphoria
The Cass review does not recommend social transition and clarifies that it is not a neutral act. Current evidence shows high levels of natural desistance if children are not socially transitioned. The SAHCS GAHG does not explain that social transition concretises cross sex gender identity in a developing child and causes socially transitioned children to persist in their cross-sex identity and progress to further medicalised interventions (a lifelong journey with major adverse effects). South African children need protection from this.
B) Puberty blockers for children and adolescents with gender dysphoria
The Cass review states that puberty blockers should only be used in the setting of a clinical trial. The harms of puberty blockers in children and adolescents are not described in the SAHCS GAHG, nor the fact that there is no good evidence available to show any benefit. South African children need protection from this.
C) Cross sex hormones for children and adolescents with gender dysphoria
The Cass review concludes that there is no high-quality evidence supporting the use of cross sex hormones in the care of young people with gender dysphoria. The SAHCS GAHG promotes unrestricted access. South African children, adolescents and young adults need protection from this.
D) Statement about a review to be undertaken for the 17 – 25yr age group
The Cass review noted that young adults aged 17-25, are also vulnerable, and harbour the same concerns as younger adolescents. The NHS has now committed to conducting a similar review in this age category, now that the Cass review has been completed.(37) The vulnerability of the 17 – 25yr age group is not mentioned in the SAHCS GAHG, nor the need to be cautious with medicalising interventions in this age group. South African young adults need a complete and through review of the evidence underpinning guidelines for caring for their transgender ideation.
E) Other conditions
The importance of managing other social and psychiatric conditions that may be a part of the cause of gender dysphoria – rather than embarking on a medicalising course – should be clearly emphasised. This is lacking in the SAHCS GAHG. South African children, adolescents and young adults need their underlying circumstances and traumas leading to their transgender ideation to be properly understood and cared for, in an evidence-based way.
Key points
Current guidelines promoting ‘gender affirming care’ for children adolescents and young adults (including the SAHCS GACG) are not based on good evidence.
There is a need for a more evidence-based approach on transgender ideation, particularly regarding children, adolescents, and young adults.
Any guideline recommending care for children, adolescents and young adults with transgender ideation must be developed by a group without conflict of interest or bias.
Social transitions are not a neutral act, and social transition concretises cross-sex identity.
Puberty blockers and cross sex hormones in children and adolescents are not supported by good medical evidence and that the harms of these treatments are severe and irreversible.
Surgical interventions cannot be advocated for at this time considering the current evidence base – especially not in children and adolescents.
Social and psychological factors (e.g. autism spectrum disorder, previous sexual assault, social contagion) that predispose to transgender ideation need to be mentioned – along with guidance on how to deal with these in counselling.
The importance of acknowledging the role of families and the exceptionally important role of parents in decision making should be emphasised.
Children and adolescents cannot consent to treatments that have severe and irreversible consequences (like reproductive sterility or loss of sexual function).
There should be inclusion of a section on the experience of the growing number detransitioners who should also be included in the conversation.
The Cass review final report that was published in April 2024 is a seismic shift in this area of medicine and has consequences for the debate in South Africa.
Proposals for possible ways forward for the SAHCS
FDNHSA would like to encourage SAHCS to review their SAHCS GAHG using the most recent and highest level of evidence and international recommendations, which expose the “gender affirming care” approach as being built on the “shaky foundations” of extremely poor-quality evidence, with the potential to cause significant harms.
Possible options for the SAHCS to consider include:
1) Retract the SAHCS GAHG guideline in full, explaining:
1.1) That the “gender affirming” approach is not based on adequate evidence.
1.2) That it is not a core function of the SAHCS to evaluate evidence or produce a guideline about care of children with transgender ideation.
2) Retract sections of the SAHCS GAHG guideline that deal with children and adolescents, explaining:
2.1) That the Cass review contains evidence that raises serious concerns about the recommendations in SAHCS GAHG for the care of South African children and adolescents with transgender ideation.
3) Review the process whereby the SAHCS came to adopt the SAHCS GAHG.
4) If deemed appropriate for the SAHCS:
4.1) Review the epidemiology and complex aetiology of transgender ideation in children, adolescents and young adults.
4.2) Establish a firm evidence base for guiding the proper care of children, adolescents and young adults with transgender ideation.
4.3) Convene a working group, including impartial research methodologists, that has no bias and no conflict of interest, to perform this task.
5) Publish a statement that the SAHCS cannot endorse its own current guidelines, this being in line with current global trends that reject the ‘gender affirming’ model, because of emergent and consolidated understanding of the evidence regarding the care of children, adolescents and young adults with transgender ideation – especially in the light of the recent publication of the final Cass review report.(1)
FDNHSA are willing to engage further with the Board of the SAHCS regarding these concerns. We await your response.
2. Taylor J, Hall R, Langton T, et al. Characteristics of children and adolescents referred to specialist gender services: a systematic review. Archives of Disease in Childhood Published Online First: 09 April 2024. doi: 10.1136/archdischild-2023-326681
3. Hall R, Taylor J, Hewitt CE, et al. Impact of social transition in relation to gender for children and adolescents: a systematic review. Archives of Disease in Childhood Published Online First: 09 April 2024. doi: 10.1136/archdischild-2023-326112
4. Heathcote C, Taylor J, Hall R, et al . Psychosocial support interventions for children and adolescents experiencing gender dysphoria or incongruence: a systematic review .Archives of Disease in Childhood Published Online First: 09 April 2024. doi: 10.1136/archdischild-2023-326347
5. Taylor J, Mitchell A, Hall R, et al. Interventions to suppress puberty in adolescents experiencing gender dysphoria or incongruence: a systematic review. Archives of Disease in Childhood Published Online First: 09 April 2024. doi: 10.1136/archdischild-2023-326669
6. Taylor J, Mitchell A, Hall R, et al. Masculinising and feminising hormone interventions for adolescents experiencing gender dysphoria or incongruence: a systematic review. Archives of Disease in Childhood Published Online First: 09 April 2024. doi: 10.1136/archdischild-2023-326670
7. Taylor J, Hall R, Langton T, et al. Care pathways of children and adolescents referred to specialist gender services: a systematic review. Archives of Disease in Childhood Published Online First: 09 April 2024. doi: 10.1136/archdischild-2023-326760
8. Taylor J, Hall R, Heathcote C, et al. Clinical guidelines for children and adolescents experiencing gender dysphoria or incongruence: a systematic review of guideline quality (part 1). Archives of Disease in Childhood Published Online First: 09 April 2024. doi: 10.1136/archdischild-2023-326499
9. Taylor J, Hall R, Heathcote C, et al. Clinical guidelines for children and adolescents experiencing gender dysphoria or incongruence: a systematic review of recommendations (part 2). Archives of Disease in Childhood Published Online First: 09 April 2024. doi: 10.1136/archdischild-2023-326500
10. Hall R, Taylor J, Heathcote C, et al. Gender services for children and adolescents across the EU-15+ countries: an online survey. Archives of Disease in Childhood Published Online First: 09 April 2024. doi: 10.1136/archdischild-2023-326348
13. Muller M, De Vries E, Tomson A, McLachlan C. An introduction to gender affirming healthcare: What the family physician needs to know. S Afr Fam Pract (2004). 2023 Jul 31;65(1):e1-e5. doi: 10.4102/safp.v65i1.5770. PMID: 37526532; PMCID: PMC10483305.
14. Tomson A, McLachlan C, Wattrus C, et al. Southern African HIV Clinicians Society gender-affirming healthcare guideline for South Africa. South Afr J HIV Med. 2021;22(1):a1229. https://doi.org/10.4102/sajhivmed.v22i1.1299
15. Tomson A, McLachlan C, Wattrus C, et al.; for the Southern African HIV Clinicians Society. Southern African HIV Clinicians Society gender-affirming healthcare guideline for South Africa – expanded version. October 2021
16. Chan Swe N, Ahmed S, Eid M, Poretsky L, Gianos E, Cusano NE. The effects of gender affirming hormone therapy on cardiovascular and skeletal health: A literature review. Metabolism Open. 2022;13:100173.
18. Sallie Baxendale. The Impact of Suppressing Puberty on Neuropsychological Function. TechRxiv. February 07, 2024. DOI: 10.22541/au.170446841.14546991/v3
24. Reinl J. Young North Carolina woman sues the doctors who put her on testosterone at age 17, saying she needed therapy, not a double mastectomy, in latest blockbuster ‘detransition’ lawsuit. Mail Online. 18 July 2023. Available at:
27. Sainz R. Susana Domínguez, the Spanish trans woman who regrets her sex change when she was a minor. VOZ Media. 25 Feb 2023. Available at: https://voz.us/susana-dominguez-the-spanish-trans-woman-who-regrets-her-sex-change-when-she-was-a-minor/?lang=en
28. COHERE (Council for the Choices in Health Care). (2020). Palveluvalikoimaneuvoston Suositus: Alaikäisten Sukupuoli-identiteetin Variaatioihin Liittyvän Dysforian Lääketieteelliset Hoitomenetelmät [Recommendation of the Council for Choices in Health Care in Finland: Medical treatment methods for dysphoria related to gender variance in minors].
29. Ludvigsson, J. F., Adolfsson, J., Hoistad, M., Rydelius, P. A., Kristrom, B., & Landen, M. (2023). A systematic review of hormone treatment for children with gender dysphoria and recommendations for research. Acta Paediatrica. https://doi.org/10.1111/apa.16791
30. National Institute of Health and Care Excellence (NICE). (2020a). Evidence review: Gender-affirming hormones for children and adolescents with gender dysphoria. Available at: https://cass.independent-review.uk/nice-evidence-reviews/
31. National Institute of Health and Care Excellence (NICE). (2020b). Evidence review: Gonadotrophin releasing hormone analogues for children and adolescents with gender dysphoria. Available at: https://cass.independent-review.uk/nice-evidence-reviews/
32. Cass H. Cass Review Interum Report. Feb 2022. Availabe at: https://cass.independent-review.uk/publications/
33. ‘Clinical Policy: Puberty suppressing hormones’. NHS England. 12 March 2024. Available at: https://www.england.nhs.uk/publication/clinical-policy-puberty-suppressing-hormones/
35. Brouwers MC et al. 2010. AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. PMID: 20603348; PMCID: PMC3001530.
36. MacRichards, L. 2019. Bias, not evidence dominates WPATH transgender standard of care; Canadian Gender Report; https://genderreport.ca/bias-not-evidence-dominate-transgender-standard-of-care/
38. Block J. Gender dysphoria in young people is rising-and so is professional disagreement. BMJ. 2023 Feb 23;380:382. doi: 10.1136/bmj.p382. PMID: 36822640.
This is the August 2024 position statement released by the SAHCS on their website: